
Updated August 8, 2022
What should we do if a student has COVID symptoms or an exposure? Click here for guidance from Alameda County.
Masks + ventilation + distancing + testing remain our most effective tools for reducing COVID transmission in schools. Vaccinations reduce the risk of severe disease.
How do we reduce COVID transmissions in schools and other indoor group settings?
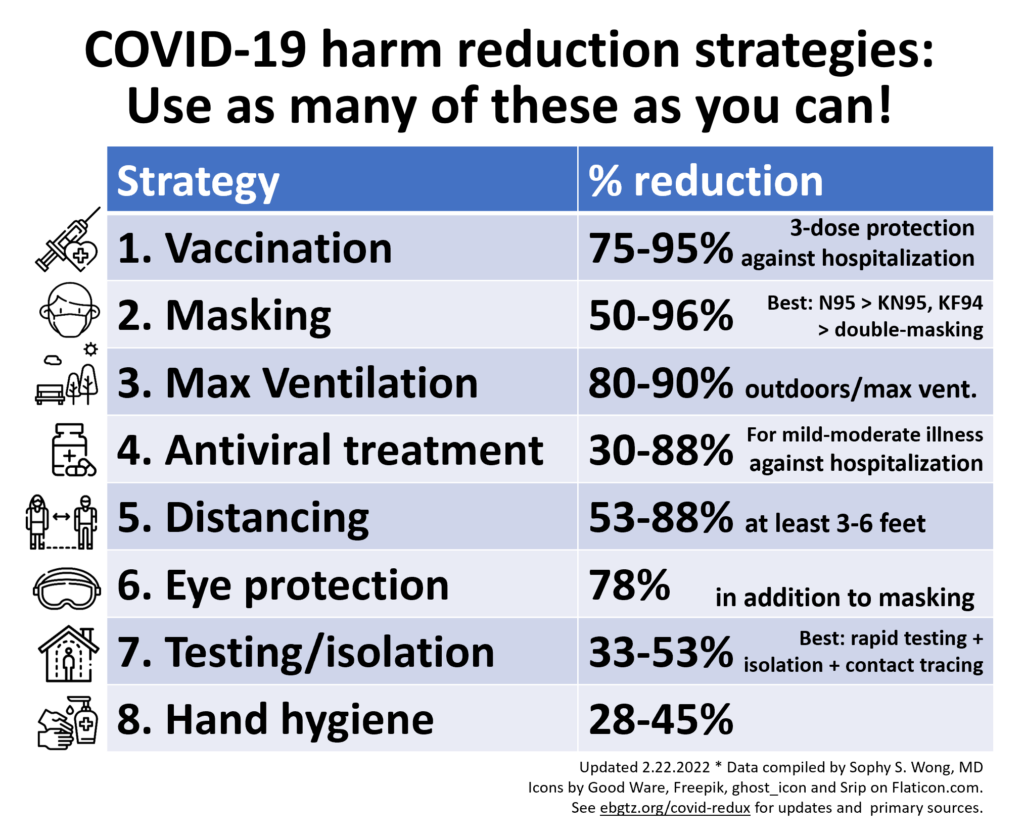
Using multiple prevention strategies together is crucial for reducing COVID-19 risk and spread. No single strategy is enough on its own, so we aim to do as many as possible with what we have. Here are the top evidence-based COVID risk reduction strategies:
- Vaccinations for everyone, including all school-aged children. CDC vaccine efficacy data during the Omicron surge shows that COVID hospitalizations for unvaccinated kids ages 5-11 years were 3x higher compared to kids who were vaccinated.
- Universal mask wearing with multi-layered masks that stay over noses and mouths and fit tight against the face (top, sides, bottom). N95s are best for adults. KF94s and KN95s are next best and come in sizes for kids and smaller faces. Double masking with a tight cloth mask over a surgical mask with all gaps closed also offers decent protection.
- Maximizing ventilation by:
- Having as many activities outdoors as possible, especially while eating/drinking, singing, shouting and exercising.
- In classrooms and other indoor spaces by:
- keeping windows and doors open for indoor/outdoor air exchange,
- running fans to increase air flow at windows and doors,
- running HVAC systems with MERV 13+ filters to clean the air, and
- running HEPA air purifiers at the maximum rate tolerable starting at least an hour before class, during class and at least an hour after class to clean the air. Here’s a DIY HEPA air filter design for a lower cost ($60-80) option.
- If the air quality is poor due to wildfires and you can’t keep windows and doors open, run the HVAC system and air purifiers at the highest settings tolerable.
- Check out these ventilation tools to see how virus particle levels change when you use different interventions, such as opening windows and using air filters or HVAC systems.
- Maximizing distance by removing non-essential furniture, placing seats 3+ feet apart, facing desks the same direction, marking “safety zones” with colorful tape to remind students to distance, and keeping classroom cohorts apart.
- Eye protection with enclosed goggles in the highest-risk settings, adding face shields to masks and/or by wearing glasses instead of contacts.
- Testing, symptom screening, staying home when sick, isolation and quarantine with routine testing at least 1-2 times per week during periods of high transmission (such as winter months), symptom screening and staying home when sick or with symptoms, contact tracing for COVID-19 cases, and quarantining or testing when exposed to COVID-19.
- Hand hygiene with frequent use of hand sanitizer and hand washing, especially before and after eating/drinking, touching faces and other people, using high-touch knobs, switches, the bathroom, playground and sports equipment.
In indoor cafeterias, in addition to maximizing ventilation as above,
- Provide additional lunch periods to reduce the numbers of students eating in the same space at the same time,
- Seat people eating 6+ feet apart and not directly facing each other, and
- Hold “quiet competitions” to minimize droplets (talking, shouting and singing) while masks are off.
The video below is of a Q&A session on COVID school safety with Lincoln Elementary teachers in Oakland on August 25, 2021. You can also download a PDF of the slides.
Detailed tools, references and key studies

- Family plan template with an example back-to-school family COVID prevention plan (downloadable doc).
- Podcast “Toolkit: Kids, School and Delta” from In the Bubble with Andy Slavitt, Dr. Peter Hotez (pediatrician and vaccinologist) and Dr. Richard Corsi (indoor/school ventilation expert).
- Maximizing mask protection:
- Mask recommendations for kids from aerosol scientists Linsey Marr, PhD and Aaron Prussin, PhD at Virginia Tech.
- Video on masking for kids under 12 and companion spreadsheet of tested kid/toddler masks including small, XS and XXS options from Aaron Collins (engineer and parent).
- Video on masking science FAQs and spreadsheet of all masks tested by Aaron Collins.
- Reducing side gaps in surgical masks using the “knot and tuck” method: picture here; video here.
- CDC’s list of trusted N95s and guide for spotting fake N95s.
- Home DIY fit-testing process from Dr. Richard Corsi, aerosol scientist and Dean of Engineering at UC Davis.
- Maximizing ventilation in schools:
- Short videos from UC Davis (the second one is more practical)
- Guidance from CDC and the EPA
- COVID cases in your local school district: check your district’s COVID dashboard.
- Oakland Unified School District COVID dashboard (go to “school level data” tab for details)
- COVID cases in kids by state and nationwide:
- California’s Safe Schools for All online hub
- COVID-19 School Data Hub from Emily Oster and team at Brown University. Read more about it here.
- The CDC has a webpage summarizing COVID-19 transmissions and prevention in schools and childcare.
Key studies on COVID-19 risk reduction in schools and youth programs
A CDC study of schools in Arkansas August–October 2021 (pre-Omicron) found that districts with universal mask requirements had a 23% lower incidence of COVID-19 among staff members and students compared with districts without mask requirements.
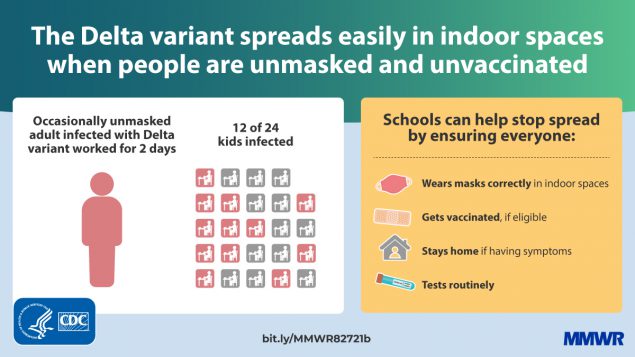
An outbreak at a Marin County elementary school in May-June 2021 (during Delta variant predominance) demonstrates the importance of vaccinations for everyone eligible and strict universal masking, in addition to ventilation, routine testing and staying home when sick. The outbreak involved an unvaccinated teacher who took off their mask to read and subsequently spread COVID to at least half their students, despite the students remaining masked and 6 feet apart, the windows and doors being open, and having an air purifier in the classroom.
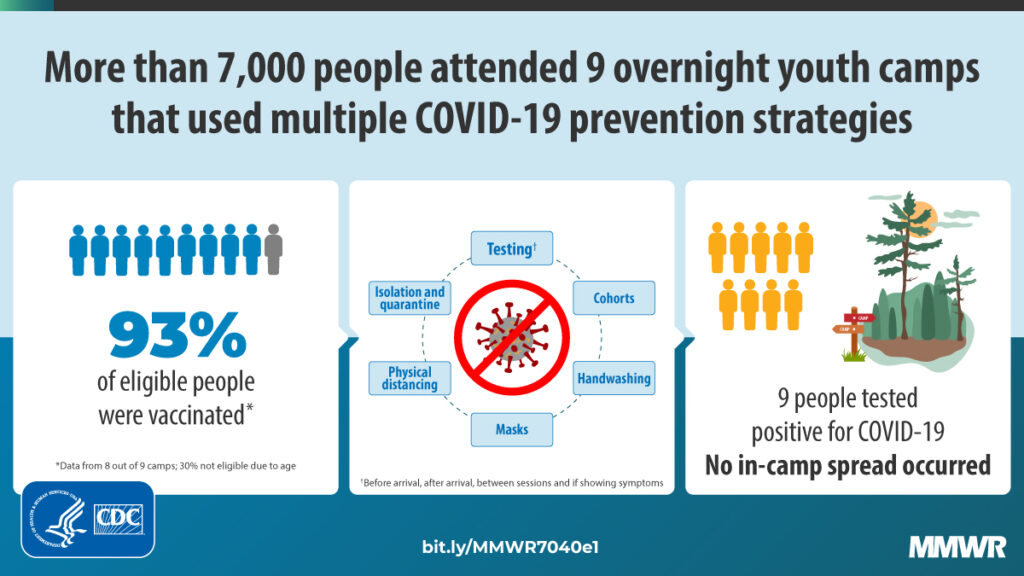
A study of over 7,000 people in overnight youth camps during the delta outbreak also showed that multicomponent strategies of high vaccination coverage (>93% among eligible people ages 12+), frequent screening and testing, masking, cohorts and other measures resulted in zero in-camp transmissions.
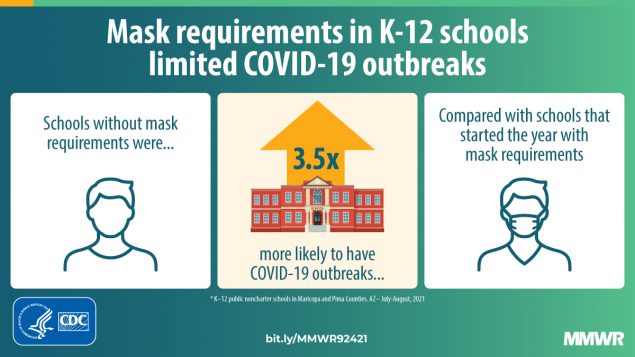
Studies on masking in schools during the delta outbreak show that mask mandates in Arizona schools reduced outbreaks by 3.5 times and nationwide reduced pediatric cases by about half.
A nationwide study of in-person schooling, mitigation measures and COVID cases and symptoms found that while there were 30% more COVID cases in household when a child was in-person at school, when a school implemented 7 or more mitigation measures, case rates matched or fell below community case rates. The most common mitigation measures used in these schools included universal mask requirements, extra space between desks, restricted entry, no supply sharing, classroom cohorts, reduced class sized and symptom screening.
A separate survey study of 6654 childcare professionals from all 50 states found that “child masking at baseline (May 22 to June 8, 2020) was associated with a 13% reduction in program closure within the following year, and continued child masking throughout the 1-year study period was associated with a 14% reduction in program closure.”
The following table summarizes a more nuanced approach to assessing risk and need to distance in different settings from BMJ, Jones et al.: “Two metres or one: what is the evidence for physical distancing in covid-19?” This article reviews the scientific evidence on physical distancing, argues that rigid distance rules are an oversimplification and offers a more nuanced model based on risk.

The largest randomized trial on the effectiveness of face masks in real-world settings, including 340,000 adults living in 600 communities in Bangladesh, showed that wearing masks, particularly surgical masks, is effective in reducing the spread of COVID-19 in community settings. The researchers’ 4-part “NORM” intervention (including no-cost/free masks, info about masks, role modeling and mask reminders) increased community mask-wearing by 3x and prevented 1 in 3 infections among people ages 60+ who are at highest risk for severe disease. Villages that used surgical-type masks had a greater reduction in symptomatic infection.
“These results suggest that we could prevent unnecessary death and disease if we get people to wear high-performance masks, such as surgical masks, in schools, workplaces, shopping centers, places of worship and other indoor spaces,” said study co-author Laura Kwong, an assistant professor of environmental health sciences at Berkeley’s School of Public Health. “I would strongly recommend that people who spend time in indoor public spaces, including students, wear surgical masks or other high-performance masks such as N95s, KN95s or KF94s. Fit and comfort are especially important for children, so child-sized KF94s may be most appropriate for them.”
More studies on safer school reopenings
California is requiring “All adults and students in K-12 school settings must wear masks indoors.” The American Academy of Pediatrics released updated guidance for schools on July 17 also recommending masks for all people ages 2 and over in school and childcare settings.
Multiple studies from 2020 have shown that schools can safely reopen with fewer transmissions than in the surrounding community when mitigation strategies with masking, distancing, cohorts, capacity limits and ventilation in place. However, current school guidance is based on studies done before the delta variant was prominent. Stricter implementation of these strategies is even more crucial during times of high community case rates and a surge in more infectious variants, like now. In a study from 2020 before Delta was widespread, British researchers found that for every five additional cases per 100,000 people in a community at large, the risk of a school outbreak increased 72%.
A study of a million students in North Carolina March-June 2021 (pre-delta) showed that proper universal masking is the most effective mitigation strategy for prevention COVID transmissions in schools when COVID-19 is circulating and students are ineligible for vaccination or uptake is inadequate. Fewer than 1% of the 40,000 in-school contacts of over 7,000 students and staff with diagnosed COVID-19 became infected while universal mask mandates were in place during a time when statewide case rates were around 15 cases/100k (5-23/100k range).
Other studies of schools in Utah, Missouri and Wisconsin showed that mask mandates were associated with lower transmissions in schools, and a study of a high school in Israel that didn’t use masks led to a large outbreak. Overall, these studies suggest a pre-delta 13% secondary attack rate in schools without masking and <1% secondary attack rate in schools with universal mask mandates.
More studies on COVID and Youth
A CDC study shows that pediatric cases, ED visits and hospitalizations increased from June to August 2021 increased for people ages 0-17. The pediatric hospitalization rates were nearly 4 times higher in states in the lowest quartile of vaccination rates compared to the states in the highest quartile vaccination rates.
Evidence from the CDC demonstrates that compared to previous strains, the delta variant infects kids and unvaccinated people at higher rates in recreational settings, especially indoors, such as in this gymnastics facility where 20% at the gym were infected and 53% of household contacts became infected.
While most new infections are mild cases among young, unvaccinated people, there is still a risk of long-term health impacts that we don’t understand yet. A new study from Norway shows that more than half (52%) of young people ages 16-30 had long COVID symptoms.
A large-scale Canadian public health study of 6,280 pediatric cases found that children ages 0 to 3 years had about 40% greater odds of transmitting COVID-19 to household contacts compared with children aged 14 to 17 years, based on pre-delta data collected between June 1 to Dec. 31, 2020.
Studies on vaccines for youth

Pfizer announced on September 20 that their COVID-19 vaccine is safe and effective for kids ages 5-11. Using a 10 µg administered 21 days apart, a smaller dose than the 30 µg dose for people ages 12+, study participants experienced side effects comparable to those experienced by older people. The data will be submitted and reviewed by the FDA and CDC. Pfizer plans to share data from the trial with children ages 2-5 and 6 months to 2 years by the end of this year. Both Pfizer and Moderna have expanded their clinical trials to increase the odds of picking up rare adverse events.
Depending on what the FDA and CDC find in the data, if the data is sufficient, accurate and shows that benefits of the vaccine outweigh the risks, we may be on track for a recommendation in mid to late October. This is welcome news in the midst of an unprecedented surge in cases across the US among children, with about a quarter million kids diagnosed each week over the past few weeks.
Data on vaccine safety and efficacy in children ages 2-4 are expected to be released and submitted to the FDA in December 2021.
Moderna and Pfizer reported data showing that their COVID-19 vaccine shows 100% efficacy in adolescents ages 12-15. With 2,260 adolescents participating in their trial, 18 people in the placebo group developed COVID-19 while none in the vaccinated group did. Blood antibody test data also show high titers of antibody responses in those who were vaccinated. On May 10th the FDA authorized use of the Pfizer vaccine for 12-15 year olds and on May 12th, the US Advisory Committee on Immunization Practices (ACIP) voted to recommend the Pfizer vaccine for 12-15 year olds.
Moderna announced on May 25 that their vaccine is 100% effective for 12-17 year olds in a clinical trial that enrolled 3,732 people ages 12 to 17, two-thirds of whom received two vaccine doses. There were no cases of symptomatic Covid-19 in fully vaccinated adolescents, the company reported. Moderna plans to submit data to the FDA for authorization in early June.
The CDC has posted a statement on rare cases of myocarditis and pericarditis following mRNA vaccines, mostly mild cases among young cismen ages 30 and younger that occur a few days after the 2nd dose. Myocarditis and pericarditis can also be clinical features of COVID-19 infection, and the risk remains higher for COVID-19 infection cardiac complications among unvaccinated people.
Trials for children ages 6 months to 11 years old have also begun for both Pfizer and Moderna vaccines. Based on data from an earlier study that assessed safety, Pfizer will give two doses of 10 micrograms each (a third of the dose given to adolescents and adults) to children ages 5-11 years, and two doses of 3 micrograms each to children ages 6 months to 5 years.
A study suggests that MIS-C was a rare complication of SARS-CoV-2 infection but disproportionately impacts young people of color. “In this cohort study of 248 persons with MIS-C, MIS-C incidence was 5.1 persons per 1 000 000 person-months and 316 persons per 1 000 000 SARS-CoV-2 infections in persons younger than 21 years. Incidence was higher among Black, Hispanic or Latino, and Asian or Pacific Islander persons compared with White persons and in younger persons compared with older persons.”
A new article shares data from Brazil and Israel suggesting that mass adult vaccination protects children. Outbreaks in a small proportion of UK’s schools still show that children are still a reservoir of circulating virus.