Variants in the East Bay
Find the latest variant proportions: Bay Area & CA (click on COVID, variants, region) | US | US wastewater | Global
In December 2023, we transitioned from monthly updates to posting practice-changing updates as needed. Please use the links above for updated variant data. Thank you!
What you need to know about Omicron subvariants:
- Symptoms and severity appear to be similar across Omicron subvariants.
- PCR and other molecular tests still work to pick up all Omicron subvariants.
- Rapid antigen tests still work, though don’t pick up the virus as well. Rapid antigen test are more accurate when you test multiple times, so consider testing at least 2-3 times, 24-48 hours apart. Omicron variants tend to replicate in the throat earlier than the nose, so consider getting throat samples, then nose samples on the same swab.
- Booster vaccines and antiviral treatment are still effective against severe disease from the newer variants.
- High-quality, fitted masks (N95, KN95, KF94s) still protect you and others from all variants.
- If you get COVID, talk to a provider about getting treatment, such as Paxlovid. Get a free virtual Covid visit here or call 1-888-897-1244.
East Bay variants from 2022 to 2023:
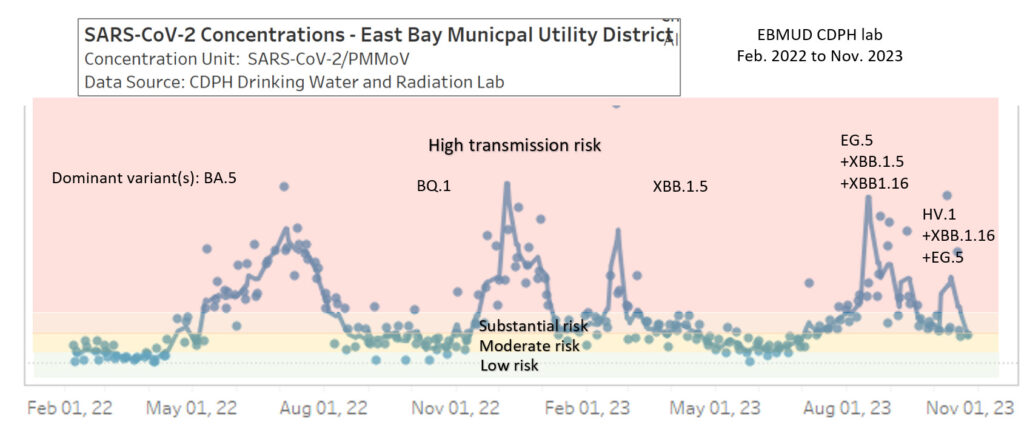
- The top 3 COVID variants in the Bay Area in November 2023 were HV.1, XBB.1.16 and EG.5, which are all descendants of XBB. California state-wide variant data (click on “COVID-19” and the “Variants” tab) shows that the BA.2 variant (presumably JN.1) is the fastest-growing variant.
- The highly mutated JN.1 variant, a descendent of Omicron BA.2.86 “Pirola”(not XBB), is rapidly spreading in Europe, Asia and Australia and has been detected in California. JN.1 is expected to be the dominant variant during winter 2023-2024.
- Data shows that updated COVID vaccines provide protection against the new variants, including the highly mutated JN.1 variant. Neutralizing antibodies for JN.1 and other circulating variants are highest for people with the updated booster and history of an XBB infection, and antibody levels are similar for people who get the booster without prior infection compared to people who had an XBB infection. This means getting a booster will increase protection for everyone, whether you had an infection or not this year.
- Get a booster to protect yourself and the community, especially if it’s been 6+ months since your last vaccine or infection. Click to find out more about vaccines and where to get them.
More info about East Bay variants circulating in 2023:
- EG.5 (nicknamed “Eris”) is another Omicron XBB subvariant with a new mutation in its spike protein that may confer immune evasiveness, hence its dominance during the late summer surge in 2023.
- HK.3 and HV.1 are descendants of EG.5.
- FL.1.5 (nicknamed “Fornax”) is also known as the variant XBB.1.9.1.1.5. It first appeared in April 2023 and has the F456L spike mutation also in EG.5 and XBB1.16.6 which confers greater transmissibility.
- XBB.1.16 (nicknamed “Arcturus”) has a transmission advantage over XBB.1.5 and was first detected in India in March 2023. It has been increasing in proportion across the US since April.
- XBB.1.5 (nicknamed “Kraken” after a mythical sea monster) was first detected in New York in December 2022 and has a mutation that virologists believe allow the virus to bind to the ACE2 receptor more tightly, making it more immune evasive and transmissible. A study of XBB.1.5 infection outcomes in New York City, the likely epicenter of XBB1.5’s emergence in the US, found that there was no evidence of increased disease severity compared to BQ.1.
How do we prepare for the next variant wave?
- Get an updated vaccine. The more doses and variant diversity your immune system is exposed to, the better it’s able to recognize new variants.
- Have a supply of high-quality masks (N95, KN95, KF94s) and carry some with you.
- Have a supply of rapid home COVID tests ready to use. Click here for information on how to get free tests through health insurance.
- Make a plan to get treatment in case you get infected.
- Have back-up plans for gatherings and travel if viral levels get too high or someone gets sick.
- Check the amount of virus in your community using the early detection wastewater surveillance US dashboard.
What are variants of concern? Why do they matter?
We have learned that SARS-CoV-2, the coronavirus that causes COVID-19, is a shape-shifting virus. Like all viruses, it mutates randomly when it replicates in someone’s body and creates new variants. When the mutations help the virus spread faster/better and spreads to others, the new variant can cause new outbreaks. These are called variants of concern.
SARS-CoV-2 has infected so many people that it has tons of chances to accumulate mutations, including ones that make it more transmissible and evade our immune systems, especially in the spike protein. We have also learned that this is a hardy virus – able to withstand a lot of mutations and still replicate and spread rapidly. We can’t predict how much new variants will be more transmissible, evade our immunity from vaccines and/or infection, escape detection from tests, remain susceptible to our treatments, or what their disease severity will be.
To manage future outbreaks from new variants, we need to keep a close watch on genomic sequencing of circulating SARS-CoV-2 strains, wastewater and case/hospitalization trends, and be ready at the earliest signs of an outbreak to rapidly implement the precautions we know that work: masking, distancing, rapid testing and isolation, and rapid access to vaccine updates and antivirals.
Click to learn more about variants in California state, the US and worldwide.
Is Omicron highly transmissible? Yes, Omicron is very contagious.
- FL.1.5 (nicknamed “Fornax”) is also known as the variant XBB.1.9.1.1.5. It first appeared in April 2023 and has the F456L spike mutation also in EG.5 and XBB1.16.6 which confers greater transmissibility.
- BA.2.86 (nicknamed “Pirola”) caused alarm in August/September 2023 because it has has 35 spike protein mutations compared to XBB1.5. However, while lab data found BA.2.86 to escape immunity from XBB by 2-3-fold, it was also ~60% less efficient at infecting cells, which may limit its transmissibility. The researchers write that BA.2.86 appears to have “traded its infectivity for higher immune evasion.”
- EG.5 (nicknamed “Eris”) is another Omicron subvariant with a new mutation in its spike protein that may confer immune evasiveness, hence its dominance during the late summer surge in 2023.
- XBB.2.3 (nicknamed “Acrux”) appears to have a transmission advantage over XBB.1.16 in India (where it was first identified) and carries the worrisome immune-evading S:T478K mutation from the Delta variant, which confers stronger viral binding to the ACE2 receptor.
- XBB.1.16 (nicknamed “Arcturus”) has a transmission advantage over XBB.1.5 and was first detected in India in March 2023. It has been increasing in proportion across the US since April.
- XBB.1.9.1 (nicknamed “Hyperion” after a moon of Saturn) has a transmission advantage over XBB.1.5 and was first detected in Southeast Asia in January 2023.
- XBB.1.5 (nicknamed “Kraken” after a mythical sea monster) has a mutation in the spike protein (F486P) that virologists believe allow the virus to bind to the ACE2 receptor more tightly, making it more immune evasive and transmissible. XBB.1.5 was first detected in New York in December 2022.
- The XBB family has 8 additional mutations and spreads even faster than BQ.1.1.
- BQ.1.1 has 6 additional key spike protein mutations that has allowed it to evade prior immunity and spread about twice as fast as BA.5.
- The BA.5 Omicron subvariant is more transmissible than the original Omicron subvariants and can reinfect people who had BA.1 infection, especially if they are unvaccinated. BA.1/2 infection does provide some immunity to BA.5 and is stronger with vaccination (~80% in one study).
- In early May 2022, South African scientists shared that two new Omicron sub-variants, BA.4 and BA.5, are causing a new surge in a population that has about 90% immunity, primarily from prior infections (in the Gauteng, Western Cape and KwaZulu-Natal provinces).
- Data from South Africa shows that the Omicron BA.5 sub-variant is more transmissible than BA.2, potentially from a combination of immune evasion (with many mutations in the spike protein) and ability to infect rapidly.
- The Omicron BA2.12.1 sub-variant is estimated to be 25% more transmissible than BA.2, which was 30%+ more transmissible than Omicron BA.1, which was 50% more transmissible than Delta, which was 80-90% more transmissible than Alpha, which was 30-50% more transmissible than the original strain.
- The original Omicron variant (BA1) is estimated to have an R0 of 4-8, which means each person who is infected with the BA1 variant is estimated to transmit the virus to 4-8 more people.
- Omicron has spread 2-3x more rapidly than Delta, as shown in data from the UK and South Africa, with cases doubling every 2-3 days, leading to explosive outbreaks.
- Omicron’s high transmissibility likely due to a combination of immune evasion, shorter incubation time (~2-3 days instead of 4 days for Delta and 5 days for older variants), and rapid replication in the upper airways (70x faster in one study).
- A CDC study found that household transmission for Omicron was 53%. Secondary attack rates were lower for people who were boosted (43%), people had their primary vaccine series (44%), compared to people who were unvaccinated (64%). People with infection who wore masks had lower transmission rates (40%) compared to those who didn’t wear masks (69%). Those who isolated also had lower transmission rates (41%) compared to those who didn’t isolate (68%).
Does Omicron evade immunity?
Yes, partially.
Do vaccines still work? Yes! Immunity wanes after 4-6 months, so be sure to get your boosters!
- Vaccines, including two doses, still work well against severe illness though not against infection. Boosters significantly increase protection. Prior infection provides less reliable immunity against Omicron compared to vaccinations and especially boosters.
- The more immunity we have built up over time, the better we are able to protect ourselves against Omicron and future variants. It’s safest and most reliable to do this with multiple vaccine doses. Infection will also add a layer of immunity, though as Omicron and Delta have shown us, a less reliable one.
- The Omicron variant has so many mutation in the spike protein that it is much better able to escape antibody immunity in the nose and mouth compared to earlier variants, including Delta. B-cell and T-cell immunity is still effective in protecting us from severe disease, but they don’t activate until after the virus enters the body, so we are more likely to get upper airway infections with Omicron compared to earlier variants.
- Data from the US shows that vaccine efficacy against hospitalization during the Omicron surge was 90% after an mRNA booster, 81% within 6 months of getting a second mRNA dose, and 57% 6+ months after a second mRNA dose. This compares to 94%, 90% and 81% respectively during the Delta surge, suggesting that the Omicron variant has mutations that confer significant immune evasion.
- A study on vaccine efficacy across 10 US states including Northern California through January 22, 2022 found that mRNA vaccine efficacy against hospitalization during the Omicron surge was 91% during the first 2 months after the booster/third dose and 78% by the 4th month.
- A large UK cohort study found that boosters gave the best protection against hospital admission from Omicron (aHR 0.22) compared to past infection alone (aHR 0.55).
- Data from the UK up to January 13, 2022 shows vaccine efficacy against hospitalizations with the Omicron variant for all brands they use (Pfizer, Moderna, Astra-Zeneca) to be 64% in the first 6 months after a second dose, 44% after 6 months of the second dose, and 92% in the first month after a booster, waning to 83% when it’s been more than 2.5 months after a booster. (Compared to 95-99% booster efficacy against hospitalization with the Delta variant.)
- A large study from New York State in January 2022 found that while the Pfizer vaccine for children 5-11 was still protective against hospitalizations with Omicron (48%), protection against infections declined rapidly (from 56% in the first 2 weeks after the 2nd dose to 12% after 2 weeks). For children aged 12, who received the higher 30 mcg dose, protection against infections was 67% (compared to 11% for children aged 11). The authors conclude: “These results highlight the potential need to study alternative vaccine dosing for children and the continued importance layered protections, including mask wearing, to prevent infection and transmission.”
- South African epidemiologists have reported more reinfections with Omicron compared to earlier variants.
Do rapid tests detect Omicron infections? Yes!
- The Unidos en Salud group in the SF Mission found that rapid antigen tests still pick up 95% of people with viral loads that are most associated with infectiousness.
- Most importantly, rapid tests will give you crucial results within 15-30 minutes of testing so you have a good idea of whether someone is currently infectious or not.
- While PCR tests are more sensitive, by the time you get the result, the person’s most infectious period may be over.
- Omicron appears to results in symptoms sooner, about a day or two after exposure, so it’s important to start isolating and test as soon as you feel symptoms.
- Omicron also appears to replicate rapidly first in the throat before the nose, so some countries (like the UK) and some people have been swabbing their throats before swabbing their noses for the rapid antigen tests (though this has not been authorized by the FDA/CDC yet). Only use the swabs that come in kits and are intended for rapid testing. Q-tips and other cotton swabs will interfere with test results.
Is Omicron less virulent (cause less severe, “milder” disease)?
Maybe, depending on your vaccine/booster status, immunity from prior infection or vaccines, demographics and comorbidities. Studies have suggested that Omicron caused less severe disease, especially compared to Delta, but one study that controlled for vaccination status, demographics and comorbidities showed that the Omicron wave was just as deadly as the Delta and Alpha waves. Kids too young to get vaccines had similar or higher hospitalization rates with Omicron compared to Delta, though this may be due to a higher proportion of children getting infected when fewer precautions (masking, testing, distancing) were used during the Omicron waves. Disease severity between the newer Omicron variants appear to be similar.
- How mild/severe Omicron infection is depends on an individual’s immune status and underlying health conditions.
- A 2023 study of XBB.1.5 infection outcomes in New York City, the likely epicenter of XBB1.5’s emergence in the US, found that there was no evidence of increased disease severity compared to BQ.1.
- A pre-print study posted in May 2022 comparing the hospitalizations and deaths in Massachusetts during the Omicron wave found that after adjusting outcomes for vaccination status, demographics and comorbidities, hospitalization and mortality risk was similar during the Omicron wave compared to the Delta and Alpha waves.
- A nationwide study found that Omicron causes less severe illness, especially among people who are vaccinated/immune (9 deaths/1,000 cases during Omicron vs. 13 deaths/1,000 cases during Delta). COVID-19 hospital stays were shorter, with fewer hospitalized people needing ICU stays, thanks to people getting vaccinated. However, case rates were 5x higher and hospitalization rates were 1.8x higher during the Omicron surge compared to the Delta surge, leading to more overall hospitalizations.
- Among adults in the US ages 65+, those who were unvaccinated were 49 times more likely to be hospitalized for COVID-19 compared to those who were boosted as of January 19, 2022.
- A large UK cohort study found that hospitalization and death rates for Omicron were much lower compared to Delta for people ages 11+ vaccinated and unvaccinated (aHR 0.41 overall for hospital admission and aHR 0.31 for death from Omicron; aHR 1.1 for kids <11 for hospital admission).
- How severe an infection depends on a person’s underlying level of immunity (how many vaccine doses, prior infection, time since vaccination or infection, etc.) and health status.
- Infection is less severe if you have a certain level of immunity, especially from vaccination and boosters.
- People who are unvaccinated and/or only have immunity from infection from an earlier variant are at higher risk for severe illness from Omicron.
- Omicron appears to stay more in the upper airways and cause less pneumonia.
- The fact that Omicron infects many more people and there are still so many unvaccinated people led to hospitals across the US still getting overwhelmed with cases during the winter surge of 2021-2022.
Is there effective treatment or PrEP for Omicron infections?
Yes, there is effective treatment for Omicron, but there is no longer effective PrEP available against the current variants as of January 2023.
- Paxlovid, remdesivir and molnupiravir are still effective as treatment against the newer variants.
- Evusheld for COVID prevention is no longer authorized due to XBB and BQ resistance.
- The monoclonal antibody COVID treatment , bebtelovimab is not effective against BQ.1/BQ.1.1 or XBB, and the FDA has withdrawn its authorization.
- Read more here.
The emergence and rapid spread of the Omicron variant reminds us of how crucial it is to get vaccines, boosters, testing, high-quality masks and good ventilation to everyone around the globe.