AIDS 2022, the International AIDS Conference, took place July 29 – August 2, 2022 in Montreal, Canada and virtually. Below are three clinical practice-changing highlights and other key studies that inform current clinical practice. For more studies and details, check out NATAP’s AIDS 2022 conference summaries and/or download the AIDS 2022 abstract book (PDF).
Practice-changing highlights from AIDS 2022:
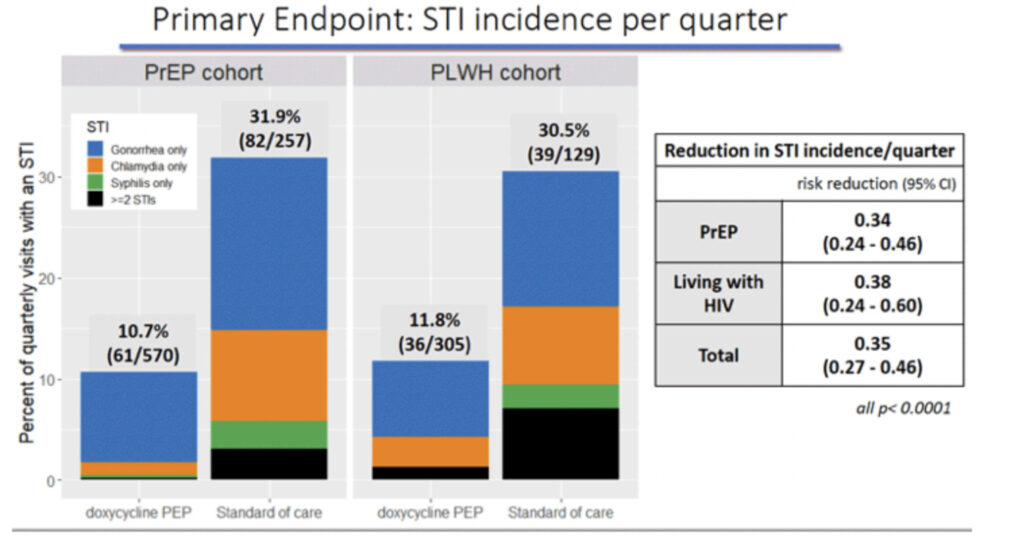
- DoxyPEP to prevent bacterial STIs: doxycycline 200 mg PO x1 within 72 hours of sex was found to reduce bacterial STIs by ~65% among MSM and transwomen living with HIV or on PrEP who’ve had at least one STI in the past 12 months and engage in condomless sex. Risk reduction for STI incidence per quarter was 0.35 overall and by STI and PrEP/PLWH respectively was 0.45/0.43 for gonorrhea, 0.12/0.26 for chlamydia and 0.13/0.23 for syphilis. See slides below. (doxyPEP study; Annie Luetkemeyer et al!)
- BIC/FTC/TAF (Biktarvy) for HBV/HIV coinfection: The ALLIANCE study (mostly in Asia and in MSM) found that people with HBV/HIV coinfection treated with BIC/FTC/TAF over DTG+F/TDF had higher rates of HBV viral load suppression, ALT normalization and HBeAg seroconversion. (ALLIANCE HBV/HIV study; Avihingsanon et al.)
- CAB/RPV (Cabenuva) for people with viremia and adherence challenges: 15 PLWH on CAB/RPV in Ward 86’s pilot group were not virally suppressed, some had advanced HIV and one had raltegravir resistance, and all achieved viral load suppression or at least 2-log drop. (CID; Kat Christopoulos et al!) Also: CAB/RPV injections in the lateral thigh had similar concentrations to gluteal injections. (Margot et al; abs. EPB240) For East Bay prescribers: Please click here for the updated Cabenuva prescribing info making the oral lead-in optional, which may help you get insurance coverage. CAB is available at specialty pharmacies, such as Community Walgreens, AHF, EBAC and AHS/Highland pharmacies.
AIDS 2022 studies that inform current clinical HIV practices:
- Cabotegravir long-acting injectable (CAB) PrEP:
- For transwomen taking hormones, CAB PrEP efficacy was comparable, and hormones don’t appear to impact CAB concentrations. During the median 1.4 years follow-up, transwomen taking CAB had lower incidence of HIV infection compared to those taking TDF/F. (HPTN 083; Grinsztejn et al.).
- Pregnancy outcomes were comparable between people taking CAB vs. TDF/FTC PrEP (HPTN 084; Delany-Moretlwe et al.).
- ART and weight gain: More studies found that TDF suppresses weight while TAF and DTG-containing regimens lead to weight gain.
- Weight gain among treatment-naïve PLWH in South Africa was most pronounced for TAF/F+DTG (9 kg) > TDF/F+DTG (6 kg) > TDF/F+EFV (3 kg) and in people who identified as females > males. (ADVANCE trial; Venter et al.)
- Dolutegravir (DTG) safety and efficacy studies affirmed first-line recommendation for all PLWH, including pregnant PLWH.
- The Pediatric HIV/AIDS Cohort study in the US and Europe found that DTG-based ART had higher rates of viral suppression at delivery (97%) compared to regimens containing elvitegravir–cobicistat (90%), raltegravir (89%), and atazanavir–ritonavir (84%). BIC+F/TAF was not studied. (NEJM; Patel et al.)
- Studies from Brazil and the NAMSAL network in Cameroon found that DTG is superior to efavirenz (EFV), especially in advanced HIV, likely related to higher rates of discontinuation of EFV due to lower tolerability. (Brites et al. and NAMSAL; Mpoudi-Etame et al.)
- The Tsepamo study in Botswana shared updated data showing that the rate of neural tube defects among babies born to people taking DTG during pregnancy was no longer higher than the rate of the general population. (Zash et al.)
- Bictegravir (BIC) 5-year follow-up shows high resistance barrier and efficacy: a US study found that pretty much everyone who takes their BIC-containing ART will stay suppressed over time, and those who didn’t did *not* develop resistance. This adds to data that show a very high resistance barrier for BIC and DTG-containing regimens. (Sax et al; abs. EPB150)
- Lenacapavir (LEN) long-acting injectable updates:
- Lenacapavir (LEN) is a long-acting injectable taken twice yearly (q6 months) studied for both HIV treatment and prevention and in a new class of HIV drugs called capsid inhibitors.
- Gilead resubmitted its LEN application for FDA approval in June 2022 and approval is anticipated by the end of 2022. The EU approved LEN on August 22.
- LEN in 72 highly treatment-experienced PLWH taking an optimized oral background regimen found that it was well-tolerated and led to high rates of viral suppression (86%) and CD4 increase. Risk factors for the 8 of 72 people who had LEN resistance poor adherence or no active background ART. (Margot et al. and VanderVeen, abs. EPB239)
- A simplified LEN regimen in which oral LEN (2 x 300mg) is given on the same day as the LEN sub-cutaneous injection (927 mg), followed by oral LEN on Day 2, found that LEN concentrations were comparable with the Phase 2/3 regimen (oral LEN on Days 1,2, 8; then injection on Day 15). (Jogiraju et al.)